
Medical schema
How to read this guide safely
This visual map connects Pelvic Floor Physiotherapy for Prostate Symptoms to anatomy, symptom triage, professional care and the limits of bodywork claims.
- 01
Observe the pattern
Sort flow, urgency, night urination, pelvic pain, ejaculation pain, PSA questions and screening anxiety.
- 02
Check red flags
Fever, chills, retention, blood, severe pain or post-procedure illness needs medical care before interpretation.
- 03
Choose the care path
Urology may use history, urine tests, PSA discussion, examination, imaging, medication or procedure review.
- 04
Keep clear boundaries
Prostate massage or supplements should never replace screening, infection care or obstruction assessment.
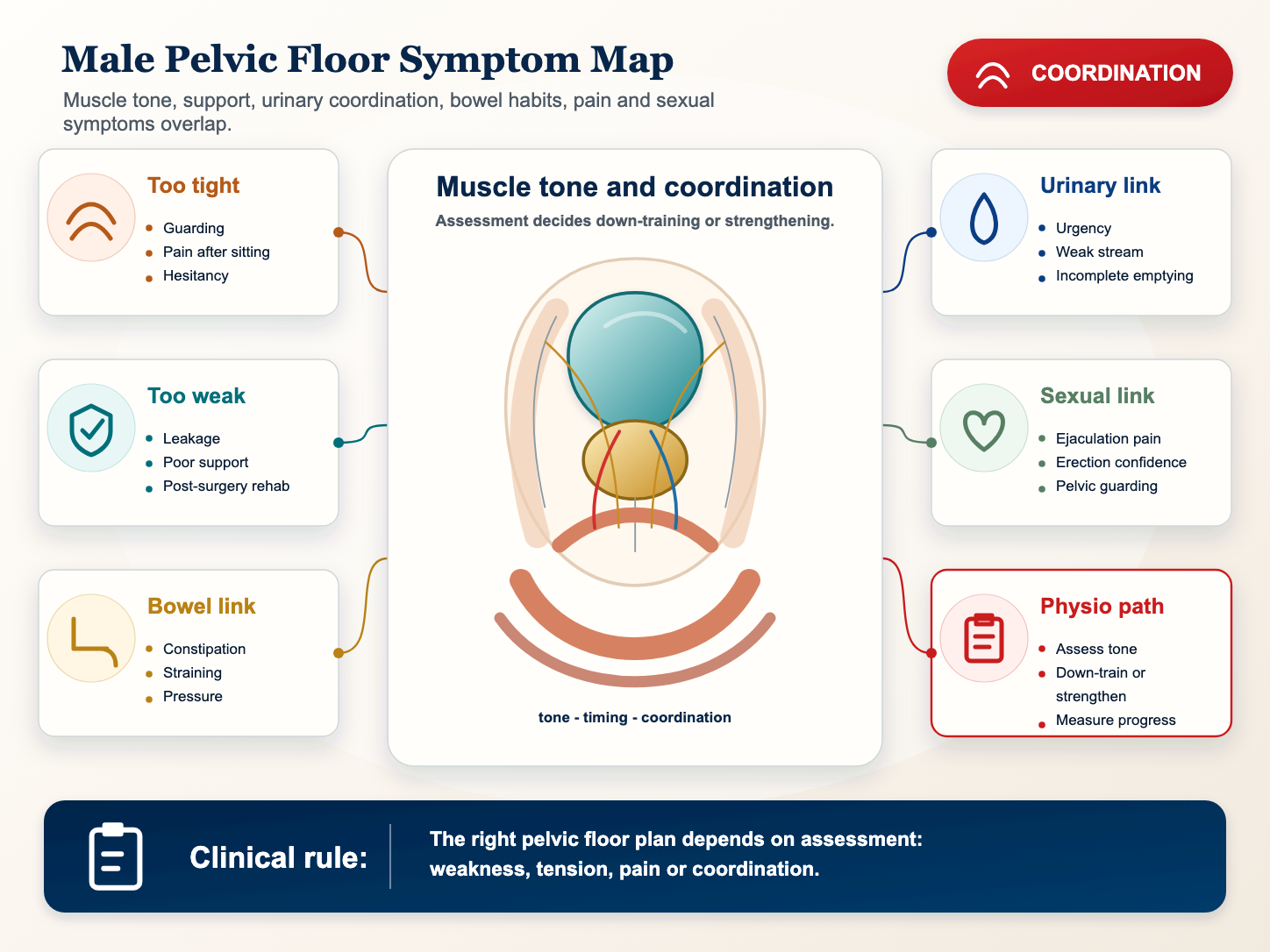
Pelvic floor physiotherapy is often misunderstood as only Kegels. For prostate-related symptoms, a qualified assessment may look at tone, coordination, guarding, breathing, bladder habits, pain behavior and recovery after treatment.
Why this guide matters
Pelvic Floor Physiotherapy for Prostate Symptoms belongs inside a larger male health map. A symptom or question rarely comes from one isolated structure. Blood flow, nerves, hormones, muscles, sleep, stress, medication, urinary habits, bowel habits and relationship context can all change how the body feels. The purpose of this page is to give a careful orientation before a reader compares treatments, bodywork traditions or online claims.
Pelvic floor physiotherapy is often misunderstood as only Kegels. For prostate-related symptoms, a qualified assessment may look at tone, coordination, guarding, breathing, bladder habits, pain behavior and recovery after treatment. The practical goal is not to diagnose from a screen. It is to improve the quality of the next decision: what to observe, what to record, what is safe to try as general wellbeing support, and what should move directly to a qualified clinician.
Simple anatomy and function
The prostate is a small gland below the bladder and in front of the rectum. It surrounds the upper urethra, contributes fluid to semen and sits close to the bladder neck, pelvic floor muscles, nerves and bowel. In plain language, the body part or system described here has a normal job, a range of normal variation and a set of warning patterns. Confusing those three categories is a common reason men either ignore important symptoms or become frightened by ordinary variation.
The pelvic floor supports the bladder and bowel and coordinates urination, continence, erection and ejaculation. It can become overactive, weak, painful or poorly coordinated around prostate symptoms or after procedures. This is why JABKASAI uses a conservative frame. Traditional language can be meaningful, but it should not replace anatomy, physiology or clinical triage. When a claim is medical, the evidence and assessment pathway must also be medical.
Common patterns to notice
Useful observation is specific. The reader should notice location, timing, intensity, triggers, duration and associated changes instead of using one vague label. For this topic, the most useful patterns include:
- Chronic pelvic pain or prostatitis-like symptoms without acute infection.
- Urinary hesitancy, urgency or leakage linked with muscle coordination.
- Pain after ejaculation, sitting or pelvic guarding.
- Recovery after prostate surgery or procedures.
- Symptoms worsened by unsupervised Kegels.
These patterns are not a home diagnosis. They are a safer way to speak with a doctor, urologist, pelvic floor physiotherapist, sex therapist or other qualified professional. Precise notes also make it harder for a practitioner or marketing page to reduce every concern to tension, blocked energy, age or anxiety.
Medical triage before interpretation
Physiotherapy should complement medical evaluation, especially when infection, cancer concern, retention or acute symptoms are possible. A serious educational page must keep this order clear. First ask whether the situation is urgent, new, severe, persistent or associated with systemic symptoms. Only after that should the reader think about lifestyle, stress, bodywork, sexual confidence or traditional wellbeing language.
Clinical assessment may involve history, physical examination, urine testing, blood testing, symptom scores, imaging, semen analysis, cardiovascular risk review, medication review or referral. The correct pathway depends on the pattern. A page can teach the map, but it cannot examine the body.
Fever, blood, urinary retention, severe sudden pain, new neurological symptoms or post-surgical complications require medical care before exercise plans.
Questions worth bringing to care
Before an appointment, write a one-page summary. It can include the first day symptoms appeared, what changed around that time, what worsens the pattern, what improves it, medication changes, sexual symptoms, urinary symptoms, bowel symptoms, fever, blood, injury, sleep, stress and previous treatments. Good questions for this topic include:
- Is the pelvic floor tense, weak, painful or poorly coordinated?
- Should exercises focus on relaxation, strength, timing or breathing?
- What signs mean the plan should pause?
- How will progress be measured without over-checking symptoms?
This kind of preparation is especially useful for intimate health because embarrassment can make appointments feel rushed. Written notes turn a private worry into clinical information. They also help separate a measurable medical question from a wellbeing preference or cultural practice.
Where lifestyle and bodywork fit
Qualified pelvic health work may include education, breathing, down-training, coordination, manual therapy or strengthening depending on assessment. Lifestyle factors such as sleep, alcohol, smoking, exercise, sitting time, metabolic health, hydration, medication, stress and relationship communication can matter, but they do not all matter in the same way for every person.
Bodywork should be described modestly. It may support relaxation, body awareness, breathing, down-regulation or comfort when the situation is non-urgent and consent is clear. It should not be sold as a cure for infection, infertility, hormone deficiency, erectile dysfunction, cancer, acute testicular pain, urinary obstruction or neurological disease. The more intimate the body area, the more important the boundaries become.
What not to assume
Do not assume Kegels are automatically good for prostatitis-like pain. Another common mistake is to assume that one normal result proves everything is fine, or that one uncomfortable sensation proves serious disease. Male intimate health often needs pattern recognition, not panic and not denial.
Readers should also avoid comparing themselves to exaggerated online stories. Sexual performance, libido, semen volume, urinary flow, pain sensitivity and energy all vary across time. A useful health page should make the reader more precise and calmer, not more ashamed or more dependent on a single technique.
Practical next step
Ask for a pelvic floor assessment when symptoms suggest muscle involvement or recovery needs a supervised plan. If symptoms are mild, stable and clearly linked with lifestyle, the next step may be observation and a routine appointment. If symptoms are sudden, severe, progressive or associated with red flags, the next step is medical care. If the concern is fertility, hormones or erectile function, objective testing usually gives a better starting point than guessing.
The bottom line is simple: understand the anatomy, describe the pattern, respect red flags, and keep wellbeing practices in their proper lane. That sequence protects both health and dignity.
How to read change over time
A single day can mislead. Male intimate health changes with sleep, hydration, stress, recent sex, exercise, bowel habits, alcohol, medication, illness and the pressure of paying attention to the symptom. A more useful pattern is built over several days or weeks. If the issue settles, stays mild and has an obvious trigger, the response can usually be calmer. If it escalates, repeats, spreads or brings new symptoms, the threshold for professional assessment should be lower.
For Pelvic Floor Physiotherapy for Prostate Symptoms, trend matters because the same symptom can sit in different categories. A mild recurring pattern may call for routine review, habit tracking or pelvic floor assessment. A sudden severe version of the same region may call for urgent care. A long-term sexual or urinary change may call for risk review and testing. The reader should avoid both extremes: ignoring change because it is embarrassing, or treating every variation as a crisis.
Professional pathway
The right professional depends on the dominant pattern. Primary care can often begin with history, examination, basic labs and referral decisions. A urologist may be needed for prostate, urinary, testicular, penile, fertility or persistent pelvic symptoms. A pelvic floor physiotherapist may help when muscle tone, coordination, sitting pain or chronic pelvic pain is part of the picture. A sex therapist or mental health professional may help when fear, avoidance, relationship pressure or mood symptoms are maintaining the cycle.
Good care does not require the reader to pick one explanation before asking for help. It is acceptable to say: this is the symptom, this is when it started, these are the triggers, these are the red flags I do or do not have, and this is what I am worried about. That kind of language lets the clinician sort the problem without forcing the reader into a label such as prostate issue, hormone issue, anxiety issue or blocked energy.
Reader checklist
- Write the first date, main location, intensity and whether the symptom is improving, stable or worsening.
- Record urinary, sexual, bowel, pain, sleep, medication and stress changes on the same page.
- Separate urgent signs from non-urgent discomfort before considering lifestyle or bodywork options.
- Ask whether objective testing would answer the question better than self-monitoring.
- Keep consent, hygiene, scope and referral rules visible if any practitioner offers bodywork.
Evidence standard and boundaries
JABKASAI uses a simple editorial standard: the more medical the claim, the stronger the evidence and clinical pathway should be. Relaxation, body awareness and comfort can be described as wellbeing outcomes. Claims about infection, fertility, testosterone, cancer, vascular disease, neurological problems, urinary obstruction or erectile dysfunction require medical evidence, testing and qualified care. A page or practitioner that blurs those categories creates risk.
This boundary is not anti-tradition. It is what allows traditional or somatic language to stay respectful without pretending to replace medicine. A reader can value touch, breath, culture, calm and privacy while still using clinicians for diagnosis and treatment. The safest position is not cynical and not gullible: appreciate wellbeing practices for what they can reasonably offer, and use medical care when the question is medical.
Professional medical sources
- NIDDK: Prostatitis and inflammation of the prostate
- NIDDK: Enlarged prostate, benign prostatic hyperplasia
- NCI: Prostate cancer screening PDQ
- NCI: PSA test fact sheet
- CDC: Prostate cancer screening
- CDC: Prostate cancer symptoms
- AUA: Male chronic pelvic pain guideline
- EAU: Chronic pelvic pain guidelines
- Cochrane: Interventions for chronic prostatitis and chronic pelvic pain
- NIDDK: Urinary retention
- NCI: Genetics of prostate cancer PDQ
- NCCIH: Saw palmetto and BPH evidence
- MedlinePlus: Male reproductive system
- NIDDK: Prostate problems
- WHO: Infertility fact sheet