
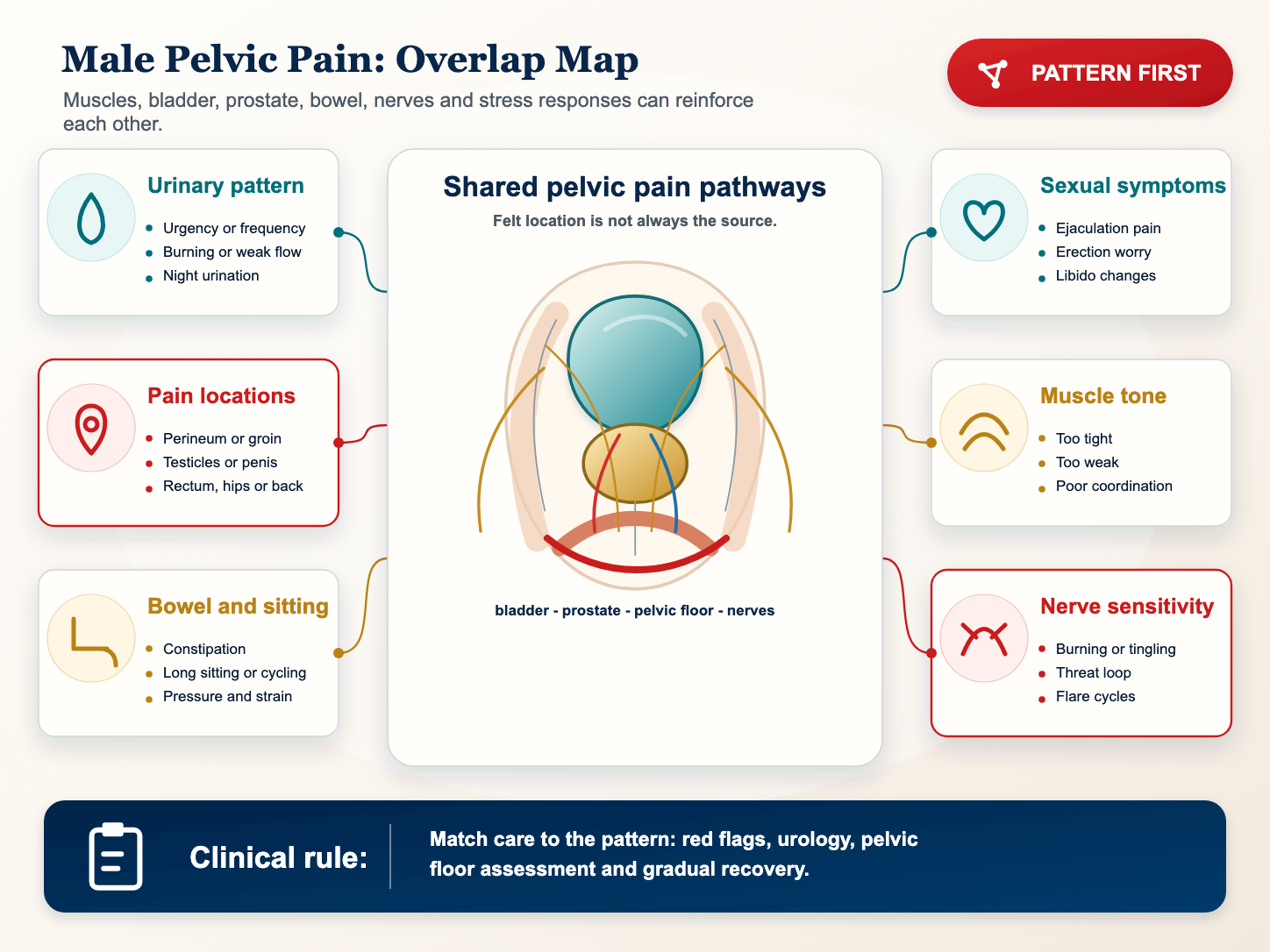
Male pelvic pain is confusing because the same region contains many systems. A man may feel discomfort in the lower abdomen, perineum, testicles, penis, rectum, groin, hips or lower back, and the sensation may change with sitting, urination, ejaculation, bowel movements, stress or exercise. It is tempting to pick one label quickly: prostate problem, muscle tightness, nerve pain, infection or anxiety. Sometimes that label is right. Often it is incomplete.
This article gives a structured way to think without self-diagnosing. Chronic pelvic pain in men can involve urology, pelvic floor muscles, bladder behavior, bowel habits, nerve sensitivity, previous infection, sexual worry, sleep and protective tension. The goal is not to make the topic bigger than it is. The goal is to stop reducing it too early. Better questions usually lead to better appointments and safer decisions.

Why the prostate gets blamed first
The prostate sits below the bladder and surrounds the urethra, so it is easy to understand why urinary symptoms make people think about it. Prostatitis, benign enlargement and other prostate conditions can cause real problems. Pain, urgency, frequency, weak stream, burning, fever or sexual symptoms should be taken seriously. But the prostate is not the only structure that can create pelvic discomfort.
A tense pelvic floor can imitate prostate symptoms. Bladder irritation, bowel dysfunction, nerve sensitization, hip or back mechanics and stress-related guarding can also contribute. This is why many modern discussions of chronic pelvic pain use a broader frame. The question is not only which organ is involved. It is also which systems keep the pattern active.
Acute prostatitis is different from chronic pain
Some patterns need quick medical attention. Fever, chills, severe urinary symptoms, blood, acute worsening or feeling very unwell are not ordinary tension patterns. Bacterial prostatitis and urinary infections can require clinical evaluation and treatment. When infection is possible, manual pelvic or prostate work is not the responsible next step.
Chronic pelvic pain is different. It may last for months, fluctuate, and involve pain without a simple positive test. That does not mean the pain is imaginary. It means the nervous system, muscles, urinary habits, bowels and stress responses may all need to be considered. A single antibiotic, supplement, stretch or massage claim may miss the complexity.
The pelvic floor can be too tense, not only too weak
Many men hear about Kegels before they hear about relaxation. That can be a problem. A weak pelvic floor and an overactive pelvic floor are not the same. Weakness may affect leakage or support. Overactivity may appear as pain, urgency, difficulty relaxing, painful ejaculation, perineal pressure or symptoms that worsen after clenching exercises. Doing more contractions can irritate some pain patterns.
A pelvic floor physiotherapist can assess tone, coordination, breathing, posture, pain behavior and urinary or bowel patterns. Treatment may include down-training, breathing, relaxation, manual therapy, education, graded activity or strengthening. The correct direction depends on the pattern. Guessing from an online exercise list is less useful than understanding whether the muscles are guarding, weak or poorly coordinated.
- Tension clues: pain with sitting, difficulty relaxing, perineal pressure, symptoms after clenching or stress flares.
- Weakness clues: leakage, poor support, post-surgical rehabilitation needs or poor timing of contraction.
- Mixed patterns are common, so assessment matters more than slogans.
Nerve sensitivity changes how pain behaves
Pain is not a simple volume knob on tissue damage. When a pain pattern persists, nerves can become more sensitive. The brain may become better at noticing signals from the pelvis, and protective muscle tension may stay active even after the original trigger has changed. This can make ordinary sitting, urination, sexual activity or stress feel connected to pain.
This does not mean the pain is psychological in the dismissive sense. It means the nervous system is part of the body. Sleep, fear, repeated checking, stress, flare cycles and avoidance can all influence sensitivity. Good care often validates the pain while also teaching ways to calm the system, restore movement confidence and reduce threat signals.
Urinary symptoms need careful notes
Frequency, urgency, weak stream, hesitancy, burning and night urination can point in several directions. They may involve prostate enlargement, infection, bladder irritation, fluid habits, medication, caffeine, anxiety, pelvic floor tension or other conditions. The most useful first step is a simple record: when symptoms occur, what the stream is like, whether there is pain, whether fever or blood appears, and what changed recently.
A clinician may use urine tests, history, examination, symptom scores or referral depending on the pattern. Notes are not a substitute for evaluation, but they make the evaluation more precise. They also help the reader avoid the common mistake of assuming that every urinary symptom is proof of prostate disease or proof that a massage technique is needed.
Sexual symptoms are part of the pattern, not a moral issue
Pelvic pain can affect erections, ejaculation, libido and confidence. Pain may make arousal feel risky. Anxiety about performance may increase pelvic guarding. Ejaculation may flare symptoms in some men. None of this should be framed as weakness or failure. It is a body system trying to protect itself, sometimes too aggressively.
The safer response is to include sexual symptoms in the medical conversation. That may feel embarrassing, but it gives the clinician or physiotherapist better information. Timing matters: did symptoms appear after infection, injury, a stressful period, a new medication, surgery, a new exercise routine or a painful bodywork session? These details help separate possible causes and maintaining factors.
Where traditional bodywork fits
Traditional bodywork may support relaxation, body awareness and a sense of care when practiced safely. It should not be presented as a universal treatment for chronic pelvic pain. If symptoms include fever, blood, severe urinary difficulty, acute testicular pain, new lumps, unexplained weight loss or major neurological changes, medical care comes first.
For non-urgent chronic patterns, the safest relationship between bodywork and medical care is complementary and modest. The practitioner should understand red flags, avoid internal or intimate claims outside scope, use informed consent, and never promise to cure prostatitis, nerve pain or erectile dysfunction. A reader should feel calmer and better informed, not pressured to choose one tradition over clinical assessment.
Why flare patterns matter
A flare is a temporary increase in symptoms. Flares can follow long sitting, cycling, heavy lifting, constipation, stress, ejaculation, a urinary infection, a new exercise plan, a painful examination or a bodywork session. The trigger does not always equal the cause, but it gives useful information. If sitting always worsens the pain, posture and nerve sensitivity may matter. If urinary burning appears with fever, infection must be considered. If symptoms spike after clenching exercises, pelvic floor overactivity may be part of the story.
The practical goal is to compare patterns rather than chase one dramatic day. A two-week log can capture intensity, location, urination, bowel movements, ejaculation, sitting time, sleep, stress and activity. That log may show that the pain is not random. It may also show that a single cure claim is too narrow. Chronic pelvic pain often improves when several small drivers are addressed together.
What multidisciplinary care can include
Multidisciplinary care does not mean that the pain is severe or hopeless. It means that the pelvis is connected to several systems. A urologist may help rule out infection, prostate disease, bladder conditions or urgent causes. A pelvic floor physiotherapist may assess muscle tone, breathing, movement and pain behavior. A primary care clinician may review medication, diabetes, sleep, mental health or bowel issues. In some cases, pain specialists, sex therapists or psychologists can help reduce fear and restore function.
The best plan is usually individualized. One person may need infection treatment. Another may need down-training, constipation support and graded activity. Another may need medication review and cardiovascular risk assessment. Traditional bodywork should not compete with this process. If it is used at all, it should be transparent, gentle, non-claiming and coordinated with the reality of the symptoms.
A practical appointment preparation method
Before seeing a clinician or pelvic floor physiotherapist, write a one-page summary. Include the main location of pain, when it started, what changed around that time, what makes it worse or better, urinary symptoms, bowel symptoms, sexual symptoms, fever, blood, injuries, surgeries, medication, exercise changes and stress or sleep patterns. Add what you have already tried and whether it helped or worsened symptoms.
This method reduces shame because it turns a private worry into clinical information. It also prevents the appointment from being consumed by vague phrases such as prostate pain or blocked energy. Precise notes do not diagnose you. They help a qualified person decide what to examine, what to test, what to treat and what to rule out.
What not to do during a flare
During a flare, many people search for the strongest intervention. That instinct can backfire. Aggressive stretching, repeated self-examination, forceful massage, excessive Kegels, long internet searches and constant checking can all increase threat and guarding. The safer first response is usually to reduce load, calm the system, record the pattern and look for red flags.
This does not mean doing nothing forever. It means matching the response to the situation. If the flare includes fever, blood, sudden testicular pain, severe urinary difficulty or neurological changes, get medical help. If it resembles a familiar non-urgent pattern, use the plan agreed with a clinician or physiotherapist. A flare is information, not an invitation to punish the body.
- Avoid testing pain with repeated pressure or stretching.
- Avoid adding strengthening exercises when the pattern suggests overactivity.
- Avoid bodywork that promises to push through pelvic pain.
What improvement should look like
Improvement is not always a sudden disappearance of pain. It may look like fewer flares, shorter flares, less fear, better sitting tolerance, improved urinary confidence, easier bowel habits, less guarding during sex or a clearer understanding of triggers. These changes can be meaningful even before the symptom is completely gone.
Tracking improvement this way helps prevent two common errors. The first is despair after one bad day. The second is chasing a dramatic cure when gradual function is returning. A good plan should make life larger over time: more movement, less avoidance, better sleep, clearer boundaries and more confidence in when to seek help.
The bottom line for chronic pelvic pain
Male pelvic pain deserves patience and structure. The prostate can matter, but it is not always the whole story. The pelvic floor can be tense or poorly coordinated. Nerves can become sensitive. Urinary, bowel and sexual symptoms can overlap. Stress and sleep can change the intensity without making the pain fake.
If symptoms are acute, severe or linked with red flags, seek medical care promptly. If the pattern is chronic and non-urgent, look for care that can coordinate urology, pelvic floor physiotherapy, pain education and lifestyle support. Avoid any practitioner or product that claims a simple cure for every pelvic symptom. Complexity is not hopeless; it is a reason to be more precise.
Fever, chills, blood in urine, severe urinary difficulty, sudden testicular pain, new neurological symptoms or acute worsening should not be handled as ordinary pelvic tension.