
ทางการแพทย์ schema
How to read this guide safely
This visual map connects Benign Prostatic Hyperplasia and ทางเดินปัสสาวะ อาการ to anatomy, symptom triage, professional care and the limits of bodywork claims.
- 01
Observe the pattern
Sort flow, urgency, night urination, อุ้งเชิงกราน อาการปวด, ejaculation อาการปวด, PSA questions and screening anxiety.
- 02
Check สัญญาณอันตราย
Fever, chills, retention, blood, severe อาการปวด or post-procedure illness needs ทางการแพทย์ care before interpretation.
- 03
Choose the care path
Urology may use history, urine tests, PSA discussion, examination, imaging, medication or procedure review.
- 04
Keep clear boundaries
ต่อมลูกหมาก massage or supplements should never replace screening, infection care or obstruction assessment.
ต่อมลูกหมากโตชนิดอ่อนโยนหรือ BPH หมายถึงการขยายตัวของต่อมลูกหมากที่ไม่ใช่มะเร็ง เป็นเรื่องปกติตามอายุ แต่ควรตีความอาการทางเดินปัสสาวะอย่างระมัดระวัง การปัสสาวะไม่ไหลและปัสสาวะตอนกลางคืนอาจเกี่ยวข้องกับต่อมลูกหมาก แต่ความเร่งด่วนและความถี่อาจเกี่ยวข้องกับพฤติกรรมของกระเพาะปัสสาวะ จังหวะการให้ของเหลว คาเฟอีน การใช้ยา เบาหวาน การรบกวนการนอนหลับ หรือความตึงเครียดของอุ้งเชิงกราน
เหตุใดคู่มือนี้จึงมีความสำคัญ
ภาวะต่อมลูกหมากโตชนิดไม่ร้ายแรงและอาการทางปัสสาวะอยู่ในแผนที่สุขภาพชายที่ใหญ่ขึ้น อาการหรือคำถามมักไม่ค่อยมาจากโครงสร้างที่แยกจากกันเพียงโครงสร้างเดียว การไหลเวียนของเลือด เส้นประสาท ฮอร์โมน กล้ามเนื้อ การนอนหลับ ความเครียด การใช้ยา พฤติกรรมการปัสสาวะ พฤติกรรมการขับถ่าย และบริบทของความสัมพันธ์ ล้วนสามารถเปลี่ยนแปลงความรู้สึกของร่างกายได้ วัตถุประสงค์ของหน้านี้คือการให้แนวทางอย่างรอบคอบก่อนที่ผู้อ่านจะเปรียบเทียบการรักษา ประเพณีกายบำบัด หรือการกล่าวอ้างทางออนไลน์
ต่อมลูกหมากโตชนิดอ่อนโยนหรือ BPH หมายถึงการขยายตัวของต่อมลูกหมากที่ไม่ใช่มะเร็ง เป็นเรื่องปกติตามอายุ แต่ควรตีความอาการทางเดินปัสสาวะอย่างระมัดระวัง การปัสสาวะไม่ไหลและปัสสาวะตอนกลางคืนอาจเกี่ยวข้องกับต่อมลูกหมาก แต่ความเร่งด่วนและความถี่อาจเกี่ยวข้องกับพฤติกรรมของกระเพาะปัสสาวะ จังหวะการให้ของเหลว คาเฟอีน การใช้ยา เบาหวาน การรบกวนการนอนหลับ หรือความตึงเครียดของอุ้งเชิงกราน เป้าหมายเชิงปฏิบัติไม่ใช่การวินิจฉัยจากหน้าจอ เป็นการปรับปรุงคุณภาพของการตัดสินใจครั้งต่อไป: สิ่งที่ต้องสังเกต สิ่งที่ควรบันทึก สิ่งที่ปลอดภัยที่จะลองใช้เป็นการสนับสนุนด้านสุขภาพโดยทั่วไป และสิ่งที่ควรส่งต่อไปยังแพทย์ที่มีคุณสมบัติเหมาะสมโดยตรง
กายวิภาคศาสตร์และฟังก์ชันที่เรียบง่าย
ต่อมลูกหมากเป็นต่อมเล็ก ๆ ใต้กระเพาะปัสสาวะและด้านหน้าไส้ตรง มันล้อมรอบท่อปัสสาวะส่วนบน ก่อให้เกิดของเหลวให้กับน้ำอสุจิ และอยู่ใกล้กับคอกระเพาะปัสสาวะ กล้ามเนื้ออุ้งเชิงกราน เส้นประสาท และลำไส้ ในภาษาธรรมดา ส่วนของร่างกายหรือระบบที่อธิบายในที่นี้มีงานปกติ มีช่วงของการเปลี่ยนแปลงปกติ และชุดของรูปแบบการเตือน การสร้างความสับสนทั้งสามประเภทนี้เป็นสาเหตุทั่วไปที่ผู้ชายเพิกเฉยต่ออาการที่สำคัญหรือรู้สึกหวาดกลัวกับการเปลี่ยนแปลงตามปกติ
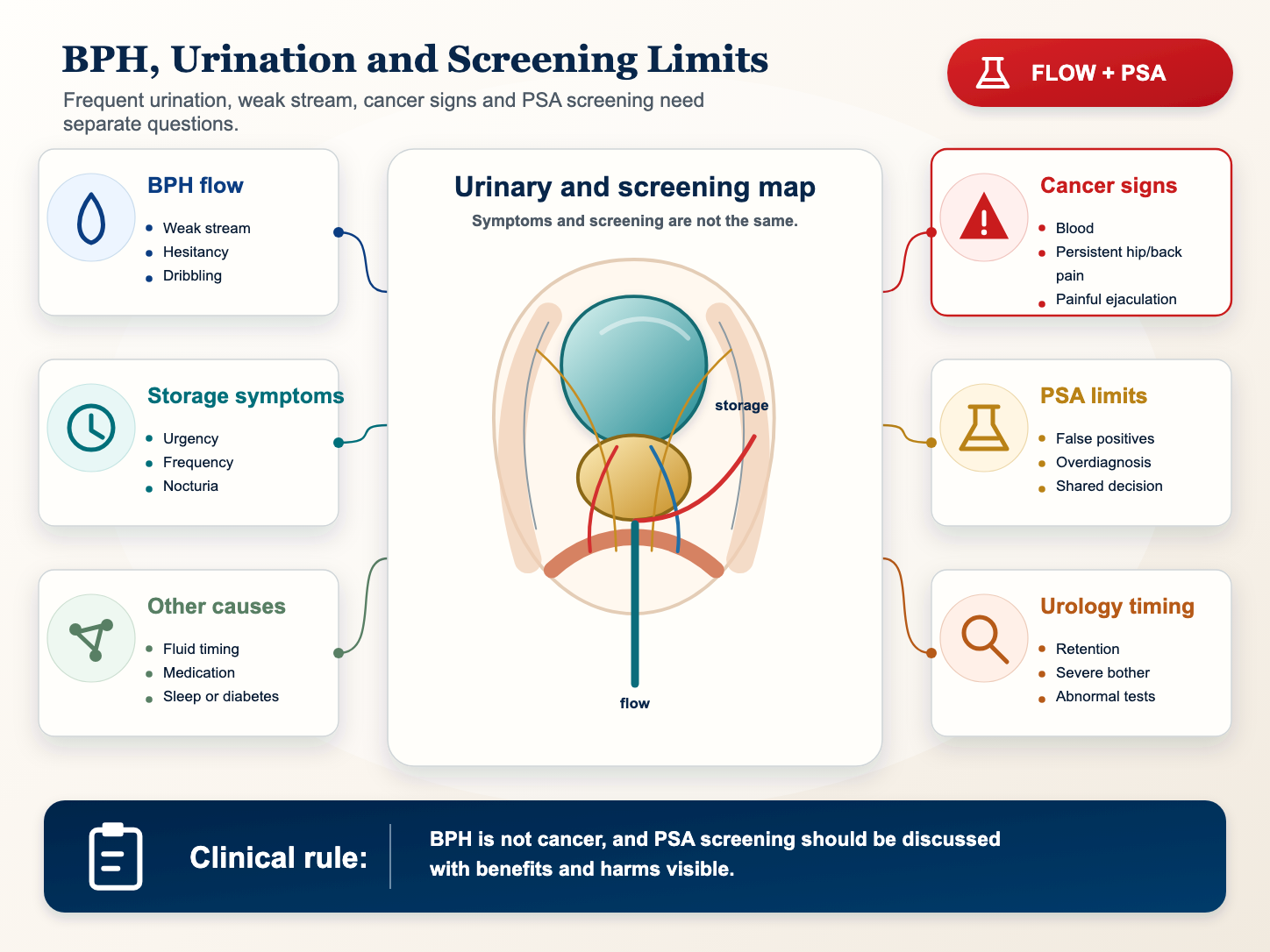
เมื่อต่อมลูกหมากขยายใหญ่ขึ้นรอบๆ ท่อปัสสาวะ อาจทำให้เกิดอาการกีดขวาง เช่น ความลังเล กระแสน้ำไหลอ่อน การไหลแบบหยุด-สตาร์ท การรัด การเลี้ยงลูกหรือการถ่ายอุจจาระไม่สมบูรณ์ อาการของการเก็บรักษา เช่น ความเร่งด่วน ความถี่ และภาวะกลางคืนอาจปรากฏขึ้นเช่นกัน แต่ไม่ได้เฉพาะเจาะจงกับขนาดของต่อมลูกหมาก การตรวจคัดกรองมะเร็งเป็นการสนทนาแยกต่างหากที่ชั่งน้ำหนักประโยชน์และโทษของ PSA ด้วยเหตุนี้ JABKASAI จึงใช้กรอบอนุรักษ์นิยม ภาษาดั้งเดิมอาจมีความหมาย แต่ไม่ควรแทนที่กายวิภาคศาสตร์ สรีรวิทยา หรือการทดลองทางคลินิก เมื่อการเรียกร้องเป็นเรื่องทางการแพทย์ หลักฐานและแนวทางการประเมินจะต้องเป็นเรื่องทางการแพทย์ด้วย
รูปแบบทั่วไปที่ควรสังเกต
การสังเกตที่เป็นประโยชน์มีความเฉพาะเจาะจง ผู้อ่านควรสังเกตสถานที่ ช่วงเวลา ความเข้มข้น สิ่งกระตุ้น ระยะเวลา และการเปลี่ยนแปลงที่เกี่ยวข้อง แทนที่จะใช้ป้ายกำกับที่คลุมเครือเพียงป้ายเดียว สำหรับหัวข้อนี้ รูปแบบที่มีประโยชน์ที่สุดได้แก่:
- ปัสสาวะบ่อย เร่งด่วน หรือตื่นตอนกลางคืนเพื่อปัสสาวะ
- กระแสน้ำอ่อน, การออกสตาร์ทล่าช้า, การไหลแบบหยุด-สตาร์ท, การเกร็งหรือการเลี้ยงบอลหลังโมฆะ
- รู้สึกว่ากระเพาะปัสสาวะไม่ว่างเปล่าหลังปัสสาวะ
- ปัสสาวะเป็นเลือดหรือน้ำอสุจิ ปัสสาวะแสบขัด การหลั่งอย่างเจ็บปวด หรือปวดกระดูกเชิงกราน/หลัง/สะโพกอย่างต่อเนื่อง
- คำถามเกี่ยวกับการคัดกรอง PSA ผลบวกลวง ผลลบลวง และการวินิจฉัยเกินเหตุ
รูปแบบเหล่านี้ไม่ใช่การวินิจฉัยที่บ้าน สิ่งเหล่านี้เป็นวิธีที่ปลอดภัยกว่าในการพูดคุยกับแพทย์ ผู้เชี่ยวชาญด้านระบบทางเดินปัสสาวะ นักกายภาพบำบัดบริเวณอุ้งเชิงกราน นักบำบัดทางเพศ หรือผู้เชี่ยวชาญที่มีคุณสมบัติเหมาะสมอื่นๆ บันทึกที่แม่นยำยังทำให้ผู้ปฏิบัติงานหรือเพจการตลาดลดความกังวลทุกอย่างเกี่ยวกับความตึงเครียด พลังงานที่ปิดกั้น อายุ หรือความวิตกกังวลได้ยากขึ้น
การคัดแยกทางการแพทย์ก่อนการตีความ
อาการทางเดินปัสสาวะควรจัดเรียงตามความรุนแรง ความรำคาญ ความเสี่ยงในการรักษา สัญญาณการติดเชื้อ เลือด บริบทการใช้ยา และความต้องการในการตรวจคัดกรองมะเร็ง หน้าการศึกษาที่จริงจังจะต้องรักษาลำดับนี้ให้ชัดเจน ก่อนอื่นให้ถามว่าสถานการณ์นั้นเร่งด่วน ใหม่ รุนแรง ต่อเนื่อง หรือเกี่ยวข้องกับอาการทางระบบ หลังจากนั้นผู้อ่านควรคิดถึงวิถีชีวิต ความเครียด การออกกำลังกาย ความมั่นใจทางเพศ หรือภาษาเกี่ยวกับความเป็นอยู่ที่ดีแบบดั้งเดิม
การประเมินทางคลินิกอาจเกี่ยวข้องกับการซักประวัติ การตรวจร่างกาย การตรวจปัสสาวะ การตรวจเลือด คะแนนอาการ การถ่ายภาพ การวิเคราะห์น้ำอสุจิ การตรวจสอบความเสี่ยงต่อโรคหัวใจและหลอดเลือด การพิจารณาใช้ยา หรือส่งต่อผู้ป่วย ทางเดินที่ถูกต้องขึ้นอยู่กับรูปแบบ หน้าเพจสอนแผนที่ได้แต่ตรวจร่างกายไม่ได้
ไม่สามารถปัสสาวะได้ มองเห็นเลือดในปัสสาวะ มีไข้พร้อมกับมีอาการทางเดินปัสสาวะ ปวดหลังหรือสีข้างอย่างรุนแรง อาการทางระบบประสาทใหม่ หรืออาการที่แย่ลงอย่างรวดเร็ว จำเป็นต้องได้รับการประเมินอย่างเร่งด่วน
คำถามที่ควรค่าแก่การดูแล
ก่อนนัดหมายให้เขียนสรุปหนึ่งหน้า อาจรวมถึงอาการวันแรกที่ปรากฏ สิ่งที่เปลี่ยนแปลงในช่วงเวลานั้น สิ่งที่ทำให้รูปแบบแย่ลง สิ่งที่ทำให้ดีขึ้น การเปลี่ยนแปลงยา อาการทางเพศ อาการทางเดินปัสสาวะ อาการลำไส้ มีไข้ เลือด การบาดเจ็บ การนอนหลับ ความเครียด และการรักษาก่อนหน้านี้ คำถามที่ดีสำหรับหัวข้อนี้ได้แก่:
- คุณปัสสาวะกลางวันและกลางคืนกี่ครั้ง?
- ปัญหาการจัดเก็บ การไหลเวียน ความเจ็บปวด เลือด หรือข้อกังวลในการคัดกรองหรือไม่?
- คาเฟอีน แอลกอฮอล์ ของเหลวตอนเย็น ยา หรือภาวะหยุดหายใจขณะหลับเกี่ยวข้องหรือไม่?
- ควรหารือเกี่ยวกับการตรวจคัดกรอง PSA ตามอายุ ความเสี่ยง และค่านิยมส่วนบุคคลหรือไม่
การเตรียมตัวแบบนี้มีประโยชน์อย่างยิ่งต่อสุขภาพของใกล้ชิด เพราะความลำบากใจอาจทำให้การนัดหมายรู้สึกเร่งรีบ บันทึกที่เป็นลายลักษณ์อักษรเปลี่ยนความกังวลส่วนตัวให้เป็นข้อมูลทางคลินิก นอกจากนี้ยังช่วยแยกคำถามทางการแพทย์ที่วัดผลได้จากความชอบด้านความเป็นอยู่ที่ดีหรือแนวปฏิบัติทางวัฒนธรรม
ที่ซึ่งไลฟ์สไตล์และตัวถังเข้ากันได้อย่างลงตัว
ขั้นตอนการใช้ชีวิตสามารถช่วยเลือกรูปแบบทางเดินปัสสาวะได้ แต่ไม่ควรส่งเสริมการนวดเพื่อรักษาสิ่งกีดขวาง การตรวจคัดกรองมะเร็ง หรืออาการทางเดินปัสสาวะที่รุนแรง ปัจจัยด้านไลฟ์สไตล์ เช่น การนอนหลับ แอลกอฮอล์ การสูบบุหรี่ การออกกำลังกาย เวลานั่ง สุขภาพการเผาผลาญ การให้น้ำ ยา ความเครียด และการสื่อสารความสัมพันธ์ ล้วนมีความสำคัญ แต่ก็ไม่ได้มีความสำคัญในลักษณะเดียวกันสำหรับทุกคน
ตัวถังรถควรอธิบายอย่างสุภาพ อาจสนับสนุนการผ่อนคลาย การรับรู้ทางร่างกาย การหายใจ การควบคุมการลง หรือความสะดวกสบาย เมื่อสถานการณ์ไม่เร่งด่วนและยินยอมอย่างชัดเจน ไม่ควรขายเป็นยารักษาโรคติดเชื้อ ภาวะมีบุตรยาก ภาวะขาดฮอร์โมน หย่อนสมรรถภาพทางเพศ มะเร็ง อาการปวดอัณฑะเฉียบพลัน ทางเดินปัสสาวะอุดตัน หรือโรคทางระบบประสาท ยิ่งบริเวณร่างกายใกล้ชิดกันมากเท่าไร ขอบเขตก็จะยิ่งมีความสำคัญมากขึ้นเท่านั้น
สิ่งที่ไม่ควรถือว่า
อย่าถือว่า BPH เป็นมะเร็ง และอย่าถือว่าอาการทางเดินปัสสาวะเป็นตัวกำหนดมะเร็งเข้าหรือออก ข้อผิดพลาดทั่วไปอีกประการหนึ่งคือการสันนิษฐานว่าผลลัพธ์ปกติหนึ่งรายการพิสูจน์ว่าทุกอย่างปกติดี หรือความรู้สึกไม่สบายใจอย่างหนึ่งพิสูจน์ว่าเป็นโรคร้ายแรง สุขภาพทางเพศของผู้ชายมักต้องการการจดจำแบบแผน ไม่ใช่ความตื่นตระหนกหรือปฏิเสธ
ผู้อ่านควรหลีกเลี่ยงการเปรียบเทียบตนเองกับเรื่องราวออนไลน์ที่เกินจริง สมรรถภาพทางเพศ ความใคร่ ปริมาณน้ำอสุจิ การไหลของปัสสาวะ ความไวต่อความเจ็บปวด และพลังงาน ล้วนแตกต่างกันไปตามเวลา หน้าสุขภาพที่เป็นประโยชน์ควรทำให้ผู้อ่านมีความแม่นยำและสงบมากขึ้น ไม่ละอายใจหรือขึ้นอยู่กับเทคนิคใดวิธีหนึ่งมากขึ้น
การปฏิบัติขั้นต่อไป
ติดตามอาการ ใช้การดูแลตามปกติสำหรับรูปแบบที่น่ารำคาญ และสอบถามแพทย์เกี่ยวกับการทดสอบ การใช้ยา ขั้นตอน หรือการตรวจคัดกรอง PSA ตามความเหมาะสม หากอาการไม่รุนแรง คงที่ และเชื่อมโยงกับวิถีชีวิตอย่างชัดเจน ขั้นตอนต่อไปอาจเป็นการสังเกตและการนัดหมายตามปกติ หากอาการเกิดขึ้นอย่างกะทันหัน รุนแรง รุนแรง หรือเกี่ยวข้องกับสัญญาณอันตราย ขั้นตอนต่อไปคือการรักษาพยาบาล หากความกังวลเกี่ยวกับการเจริญพันธุ์ ฮอร์โมน หรือการทำงานของอวัยวะเพศ การทดสอบตามวัตถุประสงค์มักจะให้จุดเริ่มต้นที่ดีกว่าการคาดเดา
สิ่งสำคัญที่สุดนั้นง่ายมาก: เข้าใจกายวิภาคศาสตร์ อธิบายรูปแบบ เคารพธงสีแดง และรักษาแนวทางปฏิบัติด้านความเป็นอยู่ที่ดีในช่องทางที่เหมาะสม ลำดับนั้นปกป้องทั้งสุขภาพและศักดิ์ศรี
วิธีการอ่านเปลี่ยนแปลงไปตามกาลเวลา
วันเดียวอาจทำให้เข้าใจผิดได้ สุขภาพทางเพศของผู้ชายเปลี่ยนแปลงไปตามการนอนหลับ การให้น้ำ ความเครียด การมีเพศสัมพันธ์ การออกกำลังกาย พฤติกรรมการขับถ่าย แอลกอฮอล์ ยา ความเจ็บป่วย และความกดดันในการใส่ใจต่ออาการ รูปแบบที่เป็นประโยชน์มากขึ้นถูกสร้างขึ้นภายในเวลาหลายวันหรือหลายสัปดาห์ หากปัญหาคลี่คลาย ไม่รุนแรง และมีสิ่งกระตุ้นที่ชัดเจน การตอบสนองมักจะสงบลง หากลุกลาม เกิดขึ้นซ้ำ แพร่กระจาย หรือทำให้เกิดอาการใหม่ เกณฑ์การประเมินโดยผู้เชี่ยวชาญควรลดลง
สำหรับอาการต่อมลูกหมากโตและอาการทางเดินปัสสาวะที่ไม่ร้ายแรง แนวโน้มมีความสำคัญเนื่องจากอาการเดียวกันนี้อาจอยู่ในประเภทที่แตกต่างกัน รูปแบบที่เกิดซ้ำเล็กน้อยอาจต้องอาศัยการตรวจสอบเป็นประจำ การติดตามนิสัย หรือการประเมินอุ้งเชิงกราน ภูมิภาคเดียวกันที่รุนแรงอย่างกะทันหันอาจจำเป็นต้องได้รับการดูแลอย่างเร่งด่วน การเปลี่ยนแปลงทางเพศหรือปัสสาวะในระยะยาวอาจจำเป็นต้องทบทวนและทดสอบความเสี่ยง ผู้อ่านควรหลีกเลี่ยงสิ่งสุดโต่งทั้งสองอย่าง: เพิกเฉยต่อการเปลี่ยนแปลงเพราะมันน่าอาย หรือถือว่าทุกรูปแบบคือวิกฤต
เส้นทางอาชีพ
มืออาชีพที่เหมาะสมจะขึ้นอยู่กับรูปแบบที่โดดเด่น การดูแลเบื้องต้นมักเริ่มต้นด้วยการซักประวัติ การตรวจร่างกาย ห้องปฏิบัติการขั้นพื้นฐาน และการตัดสินใจส่งต่อผู้ป่วย ผู้เชี่ยวชาญด้านระบบทางเดินปัสสาวะอาจจำเป็นสำหรับอาการของต่อมลูกหมาก ทางเดินปัสสาวะ อัณฑะ อวัยวะเพศชาย การเจริญพันธุ์ หรืออาการในอุ้งเชิงกรานอย่างต่อเนื่อง นักกายภาพบำบัดบริเวณอุ้งเชิงกรานอาจช่วยได้เมื่อกล้ามเนื้อ การประสานงาน อาการปวดเมื่อยจากการนั่ง หรืออาการปวดอุ้งเชิงกรานเรื้อรังเป็นส่วนหนึ่งของภาพ นักบำบัดทางเพศหรือผู้เชี่ยวชาญด้านสุขภาพจิตอาจช่วยได้เมื่อความกลัว การหลีกเลี่ยง ความกดดันในความสัมพันธ์ หรืออาการทางอารมณ์ยังคงดำเนินต่อไป
การดูแลที่ดีไม่จำเป็นต้องให้ผู้อ่านเลือกคำอธิบายหนึ่งข้อก่อนขอความช่วยเหลือ เป็นเรื่องที่ยอมรับได้ที่จะพูดว่า: นี่คืออาการ นี่คือตอนที่มันเริ่มต้น นี่คือสิ่งกระตุ้น นี่คือธงสีแดงที่ฉันทำหรือไม่มี และนี่คือสิ่งที่ฉันกังวล ภาษาประเภทนั้นทำให้แพทย์สามารถแยกแยะปัญหาได้โดยไม่ต้องบังคับให้ผู้อ่านติดป้าย เช่น ปัญหาต่อมลูกหมาก ปัญหาฮอร์โมน ปัญหาความวิตกกังวล หรือพลังงานที่ถูกบล็อก
รายการตรวจสอบผู้อ่าน
- เขียนวันแรก สถานที่หลัก ความรุนแรง และดูว่าอาการดีขึ้น คงที่ หรือแย่ลงหรือไม่
- บันทึกการเปลี่ยนแปลงของปัสสาวะ ทางเพศ ลำไส้ ความเจ็บปวด การนอนหลับ ยา และความเครียดในหน้าเดียวกัน
- แยกสัญญาณเร่งด่วนออกจากความรู้สึกไม่สบายที่ไม่เร่งด่วนก่อนพิจารณาทางเลือกในการดำเนินชีวิตหรือการออกกำลังกาย
- ถามว่าการทดสอบตามวัตถุประสงค์จะตอบคำถามได้ดีกว่าการตรวจสอบตนเองหรือไม่
- เปิดเผยความยินยอม สุขอนามัย ขอบเขต และกฎการอ้างอิงหากผู้ประกอบวิชาชีพรายใดเสนอการออกกำลังกาย
มาตรฐานหลักฐานและขอบเขต
JABKASAI ใช้มาตรฐานบรรณาธิการที่เรียบง่าย: ยิ่งมีการกล่าวอ้างทางการแพทย์มากเท่าใด หลักฐานและแนวทางทางคลินิกก็ควรจะแข็งแกร่งยิ่งขึ้นเท่านั้น การผ่อนคลาย การรับรู้ร่างกาย และความสบายสามารถอธิบายได้ว่าเป็นผลลัพธ์ด้านสุขภาพที่ดี การกล่าวอ้างเกี่ยวกับการติดเชื้อ การเจริญพันธุ์ ฮอร์โมนเทสโทสเทอโรน มะเร็ง โรคหลอดเลือด ปัญหาทางระบบประสาท การอุดตันทางเดินปัสสาวะ หรือภาวะหย่อนสมรรถภาพทางเพศ จำเป็นต้องมีหลักฐานทางการแพทย์ การทดสอบ และการดูแลที่มีคุณสมบัติ หน้าเพจหรือผู้ประกอบวิชาชีพที่เบลอหมวดหมู่เหล่านั้นจะสร้างความเสี่ยง
ขอบเขตนี้ไม่ได้ต่อต้านประเพณี เป็นสิ่งที่ทำให้ภาษาดั้งเดิมหรือภาษากายสามารถแสดงความเคารพโดยไม่ต้องแสร้งทำเป็นว่ามาแทนที่ยา ผู้อ่านสามารถเห็นคุณค่าของการสัมผัส ลมหายใจ วัฒนธรรม ความสงบ และความเป็นส่วนตัว ในขณะที่ยังคงใช้แพทย์ในการวินิจฉัยและการรักษา ตำแหน่งที่ปลอดภัยที่สุดไม่ใช่การดูถูกเหยียดหยามและไม่ใจง่าย: ชื่นชมแนวทางปฏิบัติด้านสุขภาพสำหรับสิ่งที่พวกเขาเสนอได้อย่างสมเหตุสมผล และใช้การรักษาพยาบาลเมื่อมีคำถามทางการแพทย์
เพลี้ยกระโดดสีน้ำตาลและปัสสาวะบ่อย
เพลี้ยกระโดดสีน้ำตาลสามารถตีบหรือบีบช่องท่อปัสสาวะและทำให้กระเพาะปัสสาวะทำงานหนักขึ้นเพื่อขับถ่าย เมื่อเวลาผ่านไป ผู้ชายบางคนสังเกตเห็นกระแสน้ำที่อ่อนลง รอก่อนที่กระแสน้ำจะเริ่มขึ้น การเลี้ยงลูกที่จุดสิ้นสุด หรือความรู้สึกว่างเปล่าที่ไม่สมบูรณ์ บางรายสังเกตอาการการเก็บ: เร่งด่วน ความถี่ หรือตื่นกลางดึก อาการจากการเก็บรักษาอาจก่อกวนได้มาก แต่ไม่ได้หมายความว่าต่อมลูกหมากมีขนาดใหญ่เสมอไป กระเพาะปัสสาวะ การนอนหลับ ของเหลว คาเฟอีน แอลกอฮอล์ เบาหวาน ยา และความเครียดล้วนมีส่วนช่วย
นี่คือสาเหตุที่แพทย์มักถามเกี่ยวกับทั้งการไหลและการเก็บรักษา ผู้ชายที่ตื่นขึ้นหนึ่งครั้งในเวลากลางคืนหลังจากดื่มของเหลวในตอนเย็น ต่างจากผู้ชายที่ตื่นมาหกครั้งโดยมีกระแสน้ำไม่ดีและถ่ายของเหลวไม่หมด ผู้ชายที่มีอาการแสบร้อนและมีไข้จะแตกต่างจากผู้ชายที่มีอาการอ่อนแรงตามวัยอย่างค่อยเป็นค่อยไป ผู้ชายที่มีเลือดปนในปัสสาวะต้องมีเกณฑ์ที่แตกต่างจากคนที่มีความถี่คงที่เล็กน้อย
สัญญาณมะเร็ง PSA และขีดจำกัด
มะเร็งต่อมลูกหมากอาจไม่แสดงอาการในระยะเริ่มแรก เมื่อมีอาการอาจทับซ้อนกับเพลี้ยกระโดดสีน้ำตาลและภาวะต่อมลูกหมากหรือทางเดินปัสสาวะอื่นๆ: ปัสสาวะลำบาก ไหลไม่แรงหรือหยุดชะงัก ปัสสาวะบ่อยในเวลากลางคืน ถ่ายอุจจาระลำบาก ปวดหรือแสบร้อน ปัสสาวะหรือน้ำอสุจิเป็นเลือด ปวดหลัง สะโพกหรืออุ้งเชิงกรานอย่างต่อเนื่อง และการหลั่งอย่างเจ็บปวด อาการเหล่านี้ไม่ได้พิสูจน์ว่าเป็นมะเร็ง แต่ถือเป็นข้อพิสูจน์ในการอภิปรายทางการแพทย์
PSA มีประโยชน์แต่ไม่สมบูรณ์ PSA อาจเพิ่มขึ้นพร้อมกับมะเร็ง เพลี้ยกระโดดสีน้ำตาล การติดเชื้อ อาการอักเสบ และปัจจัยอื่นๆ การตรวจคัดกรองสามารถตรวจพบมะเร็งได้ตั้งแต่เนิ่นๆ แต่ก็สามารถนำไปสู่ผลบวกลวง ภาวะแทรกซ้อนจากการตัดชิ้นเนื้อ การวินิจฉัยมากเกินไป และการรักษามะเร็งที่อาจไม่เคยเป็นอันตรายต่อบุคคลนั้น คำแนะนำในปัจจุบันเน้นการตัดสินใจร่วมกัน โดยเฉพาะสำหรับผู้ชายในช่วงอายุการตรวจคัดกรองทั่วไป โดยคำนึงถึงอายุ ปัจจัยเสี่ยง ประวัติครอบครัว และค่านิยมส่วนบุคคล
- การตรวจคัดกรองสำหรับผู้ที่ไม่มีอาการ อาการต้องได้รับการวินิจฉัย
- ค่า PSA ที่สูงไม่เหมือนกับการวินิจฉัยโรคมะเร็ง
- ค่า PSA ต่ำหรือปกติไม่ได้อธิบายทุกอาการของปัสสาวะ
- การตัดสินใจคัดกรองควรรวมถึงผลประโยชน์ อันตราย และผลที่ตามมา
แหล่งข้อมูลทางการแพทย์มืออาชีพ
- NIDDK: ต่อมลูกหมากอักเสบและการอักเสบของต่อมลูกหมาก
- NIDDK: ต่อมลูกหมากโต, ต่อมลูกหมากโตแบบอ่อนโยน
- NCI: คัดกรองมะเร็งต่อมลูกหมาก PDQ
- NCI: เอกสารข้อมูลการทดสอบ PSA
- CDC: การตรวจคัดกรองมะเร็งต่อมลูกหมาก
- CDC: อาการมะเร็งต่อมลูกหมาก
- AUA: แนวทางอาการปวดกระดูกเชิงกรานเรื้อรังในชาย
- EAU: แนวทางปฏิบัติเกี่ยวกับอาการปวดกระดูกเชิงกรานเรื้อรัง
- Cochrane: การแทรกแซงต่อมลูกหมากอักเสบเรื้อรังและอาการปวดกระดูกเชิงกรานเรื้อรัง
- NIDDK: การเก็บปัสสาวะ
- NCI: พันธุศาสตร์ของมะเร็งต่อมลูกหมาก PDQ
- NCCIH: เห็นต้นปาล์มชนิดเล็กและหลักฐานเพลี้ยกระโดดสีน้ำตาล
- MedlinePlus: ระบบสืบพันธุ์เพศชาย
- NIDDK: ปัญหาต่อมลูกหมาก
- WHO: เอกสารข้อเท็จจริงเรื่องภาวะมีบุตรยาก